Type 2 diabetes is a common chronic illness characterized by insulin resistance and eventually by decreased insulin secretion by pancreatic beta cells, leading to chronic hyperglycemia and associated long-term disease complications. In the United States, the prevalence of diabetes increased from 5.1 percent during 1988–1994 to 6.5 percent during 1999–2002.1 Like many chronic illnesses, diabetes disproportionately affects older people. It is associated with obesity, and its prevalence is higher among racial and ethnic minority populations. The annual economic burden of diabetes is estimated to be $132 billion and is increasing, mostly because of the costly complications of the disease.
Long-term complications of diabetes include microvascular disease, such as retinopathy and blindness, neuropathy, nephropathy, and end-stage kidney disease. In addition, the death rate from cardiovascular disease in adults with type 2 diabetes is two to four times as high as in adults without diabetes.2 Management of hyperglycemia using diet and pharmacologic therapy is the cornerstone of treatment for type 2 diabetes. Results from randomized controlled trials (RCTs) have demonstrated that the risk of microvascular complications, particularly retinopathy, can be reduced by improved glycemic control in patients with type 2 diabetes. However, studies have had mixed results regarding the impact of intensive glycemic control (hemoglobin A1c [HbA1c] < 7 percent) on cardiovascular events and mortality. While older studies indicated that intensive glycemic control may reduce cardiovascular morbidity and mortality, recent studies have raised the possibility that intensive glycemic control has either no effect or a negative effect on cardiovascular morbidity and mortality. These mixed results suggest the need for further research, including investigation of the long-term safety of glucose-lowering therapies. In addition to questions about optimal glycemic control, recent studies have addressed concerns about excess cardiovascular risk associated with particular oral hypoglycemic agents, specifically the risk of rosiglitazone.
In 1995, the only drugs for treating type 2 diabetes were sulfonylureas and insulin. Since then, many new pharmacotherapy options have become available. At present, there are 11 classes of diabetes medications: biguanides (i.e., metformin), thiazolidinediones, sulfonylureas, dipeptidyl peptidase-4 (DPP-4) inhibitors, meglitinides, glucagon-like peptide-1 (GLP-1) receptor agonists, an amylin analogue, bromocriptine, alpha-glucosidase inhibitors, colesevalam (a bile-acid sequestrant), and insulins. The newer agents are more costly than the older medications, and some are only approved as adjunctive therapies. In addition to having an increased number of medication choices, patients with type 2 diabetes often need to take more than one type of diabetes medication. In 2005–2006, 35 percent of all patients with diabetes were taking two classes of antidiabetes medications, and 14 percent were taking three or more classes, as compared to only 6 percent taking three or more classes in 1999–2000.
In 2007, the Agency for Healthcare Research and Quality (AHRQ) published its first systematic review on the comparative effectiveness of oral medications for type 2 diabetes, Comparative Effectiveness and Safety of Oral Diabetes Medications for Adults With Type 2 Diabetes (Comparative Effectiveness Review No. 8). The review was unique because it included comparisons of all oral diabetes medications. It also had a broad scope, including intermediate outcomes such as glycemic control and clinical outcomes such as cardiovascular disease and nephropathy, as well as adverse events. The review of 216 studies concluded that most oral diabetes medications had a similar effect on reducing HbA1c, most drugs except for metformin and acarbose caused increases in body weight, and only metformin decreased low-density lipoprotein (LDL) cholesterol. There were too few studies to make it possible to assess the differential effects of the oral diabetes medications on all-cause mortality, cardiovascular mortality and morbidity, or microvascular complications. The sulfonylurea class was associated with an increased risk of hypoglycemia, metformin with gastrointestinal problems, and the thiazolidinediones with heart failure.
In the years following publication of that review, enough studies were published to merit an update to address research gaps and integrate newer evidence. Since the first review, two new medication classes have been approved by the U.S. Food and Drug Administration (FDA). Two injectable incretin mimetics, exenatide and liraglutide, were FDA approved in 2005 and 2010, respectively. The DPP-4 inhibitors sitagliptin and saxagliptin were FDA approved in 2006 and 2009. In addition, the review needed to be updated to include evidence about combinations of medications, including combinations of an oral medication with insulin therapy.
For this update, we decided to build upon the previous evidence report by focusing on the most important issues without seeking to replicate all parts of the previous report. Thus, the current evidence report focuses on the head-to-head comparisons of medications that should be of greatest relevance to clinicians and their patients. Readers should refer to the original evidence report if they want more information about placebo-controlled trials of the medications. For the head-to-head comparisons, we conducted a comprehensive literature search that included all literature that had been searched for the first report. We expanded the scope of the review by including a few additional outcomes that were relevant to the comparisons of interest. We also included comparisons with combinations of medications. As part of the revised scope of work, we applied slightly different exclusion criteria. Therefore, this report represents both an update and an expansion of our previous comprehensive review of the evidence comparing the effectiveness and safety of oral medications used to treat type 2 diabetes.
糖尿病人食谱及忌讳 2011年AHRQ成人2型糖尿病口服药医治攻略更新
精彩推荐
- 从“标配”到“自定义”:尊界V800开启超豪华MPV个性定制新篇章

7月30日,尊界品牌正式宣布旗下旗舰MPV尊界V800全面开放个性化选配通道。作为华为深度赋能的超豪华旗舰,尊界V800自亮相以来便承载着重塑百万级MPV市场格局的重任。此次选...详细
- 《中国女性健康行业高质量发展倡议》正式发布,护舒宝携手行业共同迈向新阶段
7 月 29 日,由中国消费品质量安全促进会指导,CCTV品质信赖品牌护舒宝联合主办的中国婴幼儿及女性健康行业高质量发展主题活动在宝洁北京创新中心成功举办。护舒宝品牌与行...详细
- CNS情绪鱼油完成关键临床研究,营养干预开辟抑郁症治疗新道路
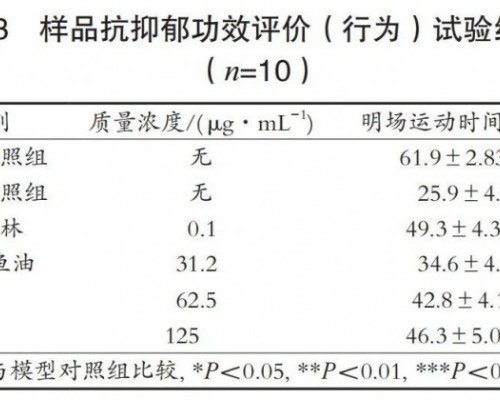
一、营养干预抑郁症治疗的诞生之源抑郁症治疗领域有一个长期存在的尴尬:药物并非对所有患者有效,副作用也十分棘手恶心、失眠、嗜睡、性功能障碍这些并非偶发,而是在相当...详细
- 从隐藏式智能电动鞋盒到卷轴星空顶,尊界MPV的野心远不止一台旗舰MPV

当个人数字生活不再满足于方寸屏幕之间的滑动,而是渴望在更广阔的空间中自由流淌时,一个移动的超级空间智能体便成为了新的向往。7月27日,随着鸿蒙智行版图扩张的号角吹...详细
本周热门
- 同仁堂健康双十一活动开启 “象食养医”倡导从健康的时候就关注健康
如果你想了解自己身体的秘密,让健康成为日常的生活方式,保持年轻的状态,实现抗衰老,逆生长的美好愿望,那么今年双十一的这场活动你一定不要错过。11月1日,同仁堂健康...详细