In the US, approximately 35% of adults with systemic lupus erythematosus (SLE) have clinical evidence of nephritis at the time of diagnosis, with an estimated total of 50–60% developing nephritis during the first 10 years of disease. The prevalence of nephritis is significantly higher in African Americans and Hispanics than in whites, and is higher in men than in women. Renal damage is more likely to develop in nonwhite groups . Overall survival in patients with SLE is approximately 95% at 5 years after diagnosis and 92% at 10 years after diagnosis (5,6). The presence of lupus nephritis (LN) significantly reduces survival to approximately 88% at 10 years, with even lower survival in African Americans.
The American College of Rheumatology (ACR) last published guidelines for management of SLE in 1999. That publication was designed primarily for education of primary care physicians and recommended therapeutic and management approaches for many manifestations of SLE. Recommendations for management of LN consisted of pulse glucocorticoids followed by high-dose daily glucocorticoids in addition to an immunosuppressive medication, with cyclophosphamide (CYC) viewed as the most effective immunosuppressive medication for diffuse proliferative glomerulonephritis. Mycophenolate mofetil (MMF) was not yet in use for LN and was not mentioned. Since that time, many clinical trials of glucocorticoids plus immunosuppressive interventions have been published, some of which are high-quality prospective trials, and some that are not only prospective but also randomized. Therefore, the ACR determined that a new set of management recommendations was in order. A combination of an extensive literature review and the opinions of highly-qualified experts, including rheumatologists, nephrologists, and pathologists, has been used to reach the recommendations. The management strategies discussed here apply to LN in adults, particularly to those receiving care in the US, and include interventions that were available in the US as of February 2012.
While these recommendations were developed using rigorous methodology, guidelines do have inherent limitations in informing individual patient care; hence, the selection of the term “recommendations.” While they should not supplant clinical judgment or limit clinical judgment, they do provide expert advice to the practicing physician managing patients with LN.
狼疮性肾炎能生孩子吗 2012年美国风湿病学会狼疮性肾炎诊治攻略
精彩推荐
- 尊界V800、尊界V680上市,双旗舰MPV开启超豪华出行新篇章

当尊界S800以连续十个月百万豪车销冠的成绩,证明中国品牌在超高端轿车领域的实力后,市场对于超豪华MPV的期待也随之升温。2026年8月5日,尊界时代旗舰MPV及华为全场景新品...详细
- 从“标配”到“自定义”:尊界V800开启超豪华MPV个性定制新篇章

7月30日,尊界品牌正式宣布旗下旗舰MPV尊界V800全面开放个性化选配通道。作为华为深度赋能的超豪华旗舰,尊界V800自亮相以来便承载着重塑百万级MPV市场格局的重任。此次选...详细
- 《中国女性健康行业高质量发展倡议》正式发布,护舒宝携手行业共同迈向新阶段
7 月 29 日,由中国消费品质量安全促进会指导,CCTV品质信赖品牌护舒宝联合主办的中国婴幼儿及女性健康行业高质量发展主题活动在宝洁北京创新中心成功举办。护舒宝品牌与行...详细
- CNS情绪鱼油完成关键临床研究,营养干预开辟抑郁症治疗新道路
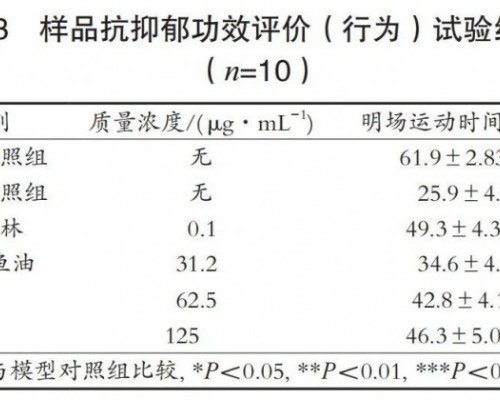
一、营养干预抑郁症治疗的诞生之源抑郁症治疗领域有一个长期存在的尴尬:药物并非对所有患者有效,副作用也十分棘手恶心、失眠、嗜睡、性功能障碍这些并非偶发,而是在相当...详细
本周热门
- 同仁堂健康双十一活动开启 “象食养医”倡导从健康的时候就关注健康
如果你想了解自己身体的秘密,让健康成为日常的生活方式,保持年轻的状态,实现抗衰老,逆生长的美好愿望,那么今年双十一的这场活动你一定不要错过。11月1日,同仁堂健康...详细